When you hear that a drug costs $500 a month, it’s easy to assume that’s just how much it costs to make. But in reality, that price often has little to do with production. It’s mostly about power-power to set prices without competition. That’s where generic competition comes in. It’s not just about cheaper pills on the shelf. It’s a powerful tool buyers-like Medicare, insurance companies, and government health systems-use to force down prices across the entire market.
Why Generic Drugs Are the Secret Weapon in Price Talks
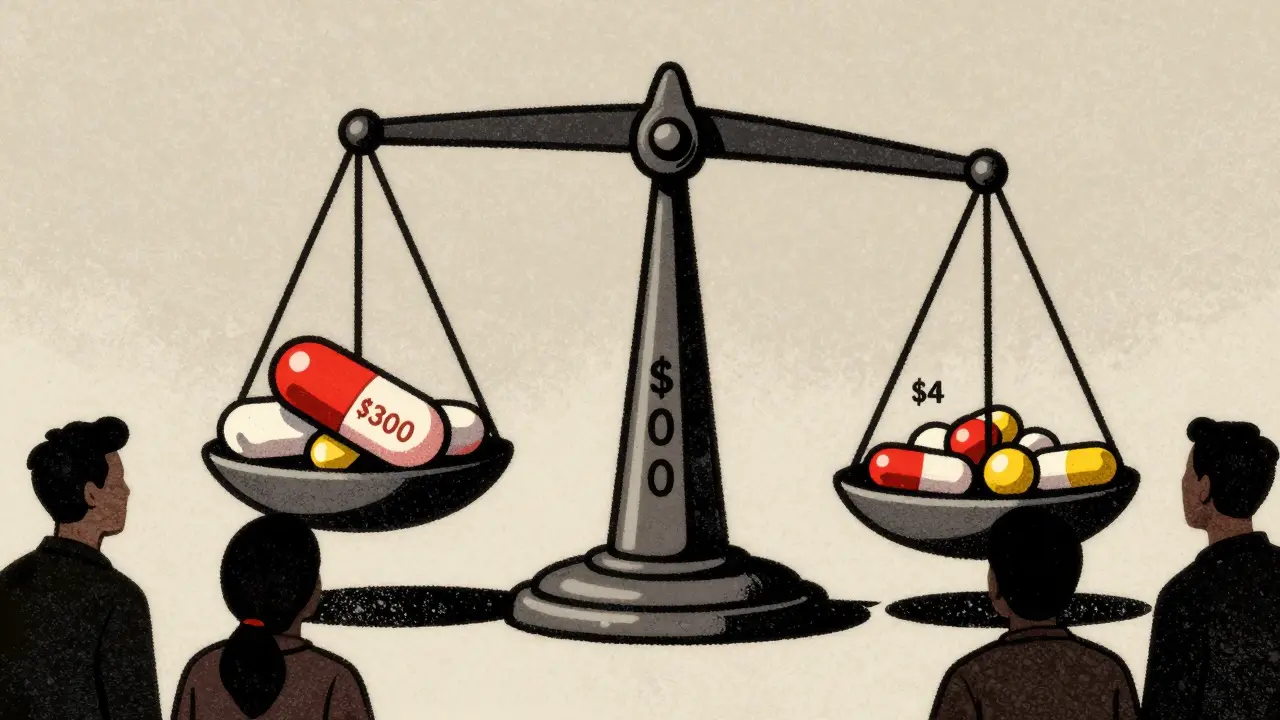
Generic drugs aren’t knockoffs. They’re exact copies of brand-name medicines, approved by the FDA after proving they work the same way. The difference? Cost. When a brand-name drug’s patent expires, generic manufacturers can enter the market. And when they do, prices don’t just drop a little-they plummet. Studies show that with just six generic competitors, prices fall by an average of 90.1%. With nine or more, they drop to 97.3%. That’s not a suggestion. That’s market physics. The more companies making the same drug, the harder they have to fight to win business. And they fight by lowering prices. This isn’t theoretical. In the U.S., generic drugs make up 90% of all prescriptions but only 22% of total drug spending. That’s because they’re cheap. A 30-day supply of a generic statin might cost $4. The brand version? $300. The gap isn’t because the brand is better. It’s because no one else is allowed to sell it yet.How Buyers Use That Competition to Negotiate
Buyers don’t just wait for generics to show up. They use the threat-or the reality-of them to negotiate before the patent even expires. The biggest player in this game? Medicare. Under the 2022 Inflation Reduction Act, Medicare can now directly negotiate prices for some high-cost drugs. But here’s the twist: they can’t negotiate with drugs that already have generic versions. Instead, they use the prices of those generics as a baseline. If a brand-name drug has five generic alternatives selling for $15 a month, Medicare won’t pay $200 for the brand. They’ll start their offer at $15-or even lower. This is called therapeutic substitution. CMS (Centers for Medicare & Medicaid Services) looks at all drugs in the same class-same chemical structure, same use, same effect-and averages their prices. That average becomes the starting point for negotiation. It’s not about what the drug costs to make. It’s about what the market already proves it’s worth. Private insurers and pharmacy benefit managers (PBMs) do the same thing, but behind closed doors. Their algorithms track every generic that enters the market, every price drop, every patent challenge. They use that data to pressure brand manufacturers into discounts before they even get to the negotiating table.How Other Countries Do It Better
The U.S. isn’t the only country using generic competition to control costs-but some do it more systematically. Canada uses a tiered pricing model. When a drug has no generics, the government allows a higher price. But as more generics enter-say, from one to three to five-the maximum allowable price drops. It’s like a sliding scale based on competition. The more players, the lower the cap. That keeps generics motivated to enter the market because they know the price will stay profitable. Germany and the UK use reference pricing. They pick a benchmark price based on the cheapest effective drug in a category. If you want to sell a more expensive version, you pay the difference yourself. Patients get the cheapest option unless they pay extra. That pushes manufacturers to compete on price, not marketing. The U.S. is starting to catch up. CMS’s 2023 guidance on drug negotiations is over 60 pages long, detailing exactly how they calculate therapeutic alternatives, what data sources they use (like Average Manufacturer Prices and Prescription Drug Event records), and how they adjust for clinical differences. It’s not perfect-but it’s a blueprint.
The Hidden Battle: How Brand Companies Fight Back
Brand-name drugmakers don’t sit back and let generics win. They’ve built entire strategies to delay competition. One common tactic? Product hopping. That’s when a company slightly changes a drug-say, switches from a pill to a capsule-and then pushes patients to the new version. The old version loses patent protection, but the new one gets a fresh 20-year clock. Between 2015 and 2020, there were over 1,200 of these moves, according to the FTC. Another? Reverse payments. A brand company pays a generic manufacturer to stay out of the market. The FTC found over 100 of these deals between 2010 and 2020. One case involved a drug called AndroGel. The brand paid the generic maker $150 million to delay entry for 10 years. That’s not competition. That’s bribery. And then there’s the rise of authorized generics. The brand company itself launches a generic version-usually at a lower price-to scare off real competitors. It looks like competition, but it’s still the same company controlling the market. The FDA calls this “strategic entry.”Why This Matters for Real People
This isn’t just about corporate profits. It’s about whether someone can afford their insulin, their blood thinner, or their heart medication. Medicare beneficiaries could save $6.8 billion a year just from the first 10 drugs negotiated under the Inflation Reduction Act. That’s real money. For someone on a fixed income, $500 a month for a drug they need is the difference between taking it or skipping doses. But here’s the catch: if government price setting happens too early-before generics even enter the market-it can backfire. A 2025 analysis by Matrix Global Advisors found that if Medicare sets a low price before generics arrive, those generics may never come. Why? Because they can’t make enough profit to cover their costs. That’s called a “chilling effect.” The goal isn’t to kill innovation. It’s to stop monopolies. The Association for Affordable Medicines says generics have lowered drug prices for over 40 years. That’s not a fluke. It’s the result of competition.
The Future: Complex Drugs and New Challenges
Not all drugs are created equal. Traditional generics-like metformin or lisinopril-are easy to copy. But newer drugs, like biosimilars (copies of biologic drugs made from living cells), are much harder and more expensive to produce. Biosimilars only have a 45% market share on average, compared to 90% for traditional generics. Why? Higher costs. Longer approval times. More regulatory hurdles. And fewer manufacturers willing to take the risk. That means the old formula-more competitors = lower prices-doesn’t work as well here. Health systems are starting to use real-world evidence to judge value. If a biosimilar works just as well but costs less, they push for it. But that’s still new. Most systems aren’t ready to use it yet. The next big push? The EPIC Act. It would delay Medicare price negotiations for small-molecule drugs until after generic competition has had time to develop. That way, generics get a fair shot. And patients get the lowest possible price.What’s Working-and What’s Not
Here’s the bottom line:- Works: Letting generics enter freely. Using their prices as a benchmark. Rewarding competition, not monopolies.
- Doesn’t work: Paying generic makers to stay away. Delaying entry with patent tricks. Setting prices before competition can even begin.
What You Can Do
If you’re a patient, ask your pharmacist: “Is there a generic version?” If you’re on Medicare, check if your drug is on the negotiation list. If you’re a policymaker, support laws that speed up generic approval and ban reverse payments. The system isn’t broken. It’s just being manipulated. And the fix is simple: more competition. More generics. Lower prices.How do generic drugs lower the price of brand-name drugs?
Generic drugs lower brand-name prices by creating real competition. When multiple companies can sell the same drug, they compete on price. This forces the brand manufacturer to lower their price to stay competitive. Even the threat of a generic entering the market can push a brand to offer discounts before the patent expires.
What is therapeutic substitution in drug pricing?
Therapeutic substitution means using the prices of similar, lower-cost drugs as a benchmark to set the price of a more expensive one. For example, if Medicare finds five generic versions of a brand-name drug selling for $10-$15, they use that range as the starting point to negotiate the brand’s price-even if the brand is still under patent. It’s not about replacing the drug, but using market data to set a fair price.
Why do some generic drugs still cost a lot?
Some generics stay expensive because there’s little competition-maybe only one or two manufacturers make the drug. Others are complex to produce, like injectables or inhalers, which require more advanced manufacturing. In some cases, brand companies launch their own “authorized generic” to block competitors. And if the market is too small, manufacturers won’t bother entering at all.
Can the government set drug prices too low for generics to enter?
Yes. If a government sets a price for a brand-name drug before any generics enter the market, it can make it impossible for generic companies to profit. They’d be competing against a government-set price, not just the brand. That’s called a “chilling effect.” Studies show this can delay or prevent generic entry, which hurts long-term savings.
What’s the difference between a generic and a biosimilar?
Generics are exact copies of small-molecule drugs made from chemicals. Biosimilars are similar-but not identical-copies of complex biologic drugs made from living cells. They’re harder to produce, cost more to develop, and take longer to approve. As a result, biosimilars have only about 45% market share, while generics reach 90%.
How can I find out if my drug has generic alternatives?
Ask your pharmacist or check the FDA’s Orange Book, which lists approved generic versions of brand-name drugs. You can also use tools like GoodRx or RxSaver to compare prices between brand and generic versions. If a generic exists, it’s almost always cheaper-and just as effective.


Jacob Hill
January 17, 2026 AT 21:31Wow, this is exactly why I started asking my pharmacist about generics-turns out my $400 insulin was $12 as a generic, and I had no idea.
It’s not even close to the same cost, and yet, same pill.
Why do we let companies get away with this? It’s not just greed-it’s systemic manipulation.
And don’t even get me started on authorized generics-brand companies playing both sides?!
It’s like a casino where the house owns every table, and the dealer’s wearing two hats.
I’ve seen this in my own family-my dad skipped doses because he couldn’t afford the brand, then found out the generic worked better because it didn’t have the same fillers.
Who even decides what’s a “filler” anyway?
And why is the FDA letting them get away with sneaky patent extensions?
Product hopping? That’s not innovation-that’s legal fraud.
And don’t tell me “it’s the market”-the market’s rigged.
Real competition would mean more than five companies making the same drug, not one company owning three of them through shell corporations.
Why do we keep pretending this is capitalism when it’s just monopoly theater?
It’s not about innovation anymore-it’s about delaying the inevitable until the patent clock runs out.
And the worst part? We’re the ones paying for it-with our health, our wallets, and our trust.
Someone needs to start holding these CEOs accountable-not just Congress, but the public too.
Jackson Doughart
January 18, 2026 AT 03:33While the economic rationale underpinning generic competition is both sound and empirically validated, one must also acknowledge the nuanced interplay between market dynamics and regulatory architecture.
The notion that price suppression through volume competition constitutes a legitimate public policy lever is not without precedent in pharmaceutical economics.
Nevertheless, the premature imposition of price ceilings-prior to the maturation of generic entry-risks undermining the very incentive structures that facilitate innovation and market entry.
It is not the existence of competition that is flawed, but rather the timing and granularity of its regulation.
One might draw parallels to the early days of broadband infrastructure: premature price controls discouraged investment, while patient, market-responsive frameworks eventually yielded robust, affordable access.
Similarly, the EPIC Act’s temporal approach-delaying negotiation until after generic competition has had opportunity to establish itself-reflects a more sophisticated, less disruptive model of intervention.
One must be cautious not to confuse market distortion with market correction.
True competition is not achieved by fiat, but by enabling conditions-clear regulatory pathways, reduced approval latency, and the absence of anti-competitive pay-for-delay schemes.
These are the levers worth pulling-not arbitrary price caps.
Tracy Howard
January 19, 2026 AT 18:56U.S. is such a joke.
Canada’s been doing tiered pricing since the 90s and we’re still arguing about whether generics are ‘real’ medicine?
Our government doesn’t let pharma run the show-we make them compete or shut up.
And you know what? We get the same drugs, cheaper, and people don’t go bankrupt taking insulin.
Meanwhile, Americans are still falling for the ‘but innovation!’ excuse like it’s 2003.
Sorry, but if your ‘breakthrough’ drug costs $500 a month and has a $4 generic alternative, you didn’t invent medicine-you invented a money printer.
Stop pretending you’re heroes. You’re rent-seekers.
And no, I don’t care if your ‘research’ cost $2 billion-your shareholders got paid 10x that in dividends.
Get a clue, America. We’re not your guinea pigs.
Valerie DeLoach
January 20, 2026 AT 08:12It’s fascinating how we’ve normalized the idea that life-saving medication should be a commodity subject to market volatility.
When we treat health as a transaction rather than a right, we create systems where profit dictates access.
Generics aren’t just cheaper-they’re a moral correction.
They force us to ask: Why does this pill cost 100x more than its chemical components?
Because we allowed patents to become monopolies, not incentives.
And now we’re surprised when companies game the system?
Reverse payments? Product hopping? Authorized generics?
These aren’t loopholes-they’re features of a broken model.
What’s more troubling is how little the public understands this.
We blame the pharmacy, the insurance, the doctor-never the structure.
But the structure is designed this way.
And yet, when we see someone choosing between insulin and groceries, we call it a tragedy.
It’s not a tragedy-it’s policy failure.
Real reform isn’t about negotiating prices-it’s about dismantling the architecture of exploitation.
Generics are the symptom of a system that forgot its purpose.
Our goal shouldn’t be lower prices-it should be dignity.
And dignity doesn’t come from a discount-it comes from justice.
Christi Steinbeck
January 22, 2026 AT 07:35THIS. IS. EVERYTHING.
I’ve been on a blood thinner for 7 years and the brand was $800 a month.
Generic? $12.
Same exact chemical.
Same exact results.
And people still think brand = better?
It’s mental.
And the fact that Medicare can now negotiate? That’s huge.
But don’t let them delay it too long-wait for generics to show up, then negotiate? No.
Let generics come in FIRST, then use their price as the floor.
Don’t let pharma play the ‘we need to protect innovation’ card while they’re literally paying competitors to stay away.
Stop the reverse payments. Ban product hopping. Make biosimilars faster to approve.
And if you’re reading this? Ask your pharmacist. Always.
You’re not being cheap-you’re being smart.
And you deserve to live without financial ruin just to stay alive.
Erwin Kodiat
January 22, 2026 AT 11:06I’ve always thought of drug pricing like buying a car.
Brand new Tesla? $80k.
Same car, 5 years later, 30k miles, no issues? $25k.
But with drugs, the ‘used’ version is just as good, but costs 1/20th.
And yet we act like the new one is somehow magically better.
It’s not.
And the fact that companies pay generics to not show up? That’s like Tesla paying Ford to not make electric cars.
It’s absurd.
And honestly? I don’t get why we don’t just make all drugs generic after a few years.
Why does anyone need to pay $300 for a drug that’s been around for 15 years?
It’s not innovation.
It’s just greed with a lab coat.
Jake Rudin
January 22, 2026 AT 11:56Let’s be honest: the real villain isn’t Big Pharma-it’s the FDA’s approval backlog.
It takes 5–7 years to get a generic approved, while patents last 20.
That’s not competition-it’s a waiting game rigged by bureaucracy.
And then they wonder why companies delay entry?
Because the system is designed to fail.
Why not fast-track generics for high-demand, low-complexity drugs?
Why not cap review times?
Why do we treat drug approval like a slow dance instead of a public health emergency?
And biosimilars? Same problem.
They’re not hard to make-they’re hard to approve.
Regulators need to stop treating every new drug like it’s a space shuttle.
It’s a pill.
It’s not rocket science.
It’s regulatory inertia.
And we’re paying for it-with our lives.
Lydia H.
January 23, 2026 AT 02:56My grandma took a generic blood pressure med for 12 years.
Never had a problem.
Switched to the brand when her insurance changed-got dizzy, nauseous, confused.
Switched back to generic-fine again.
Turns out, the brand had a different filler that didn’t agree with her.
So yeah-generics aren’t always perfect.
But they’re not the enemy.
The enemy is pretending they’re interchangeable without testing.
And the bigger enemy? Letting corporations decide who gets to live based on what they can afford.
We’re better than this.
We just have to choose to be.
Astha Jain
January 23, 2026 AT 18:13generic = cheap = bad?? no no no
in india we have generics for everything and they work fine
my uncle got cancer meds for $20/month instead of $2000
same drug
same results
but america? you pay for the logo
and then you wonder why you’re broke
pharma companies are the real scam
and the government lets them
so sad