Have you ever woken up with a tingling sensation in your pinky finger that just won't go away? Or maybe you've dropped a coffee mug because your grip suddenly felt weak. If this sounds familiar, you might be dealing with ulnar neuropathy, which is a common condition where the ulnar nerve gets compressed or pinched, leading to pain, numbness, and weakness in the hand and arm. It’s not just a minor annoyance; if left untreated, it can lead to permanent muscle loss. The good news? Most people find relief without surgery, but knowing exactly what to do-and when-is key.
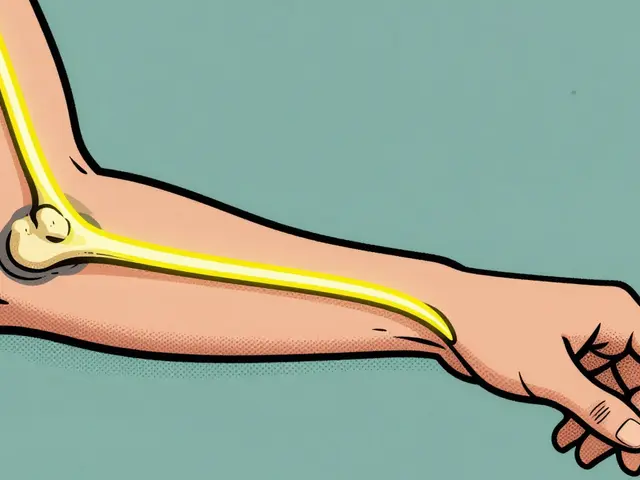
The ulnar nerve is one of the three major nerves supplying your hand. It starts near your neck, runs down your arm, passes behind the bony bump on the inside of your elbow (often called the "funny bone"), and continues into your wrist. When this nerve gets squeezed at any point along its path, the signals traveling to your fingers get disrupted. This results in the classic symptoms we’re about to discuss. Understanding where and why this happens is the first step toward fixing it.
Where Does the Ulnar Nerve Get Pinched?
Most cases of ulnar nerve entrapment happen in two specific spots: the elbow and the wrist. Knowing which area is affected helps determine the right treatment plan.
Cubital Tunnel Syndrome is the compression of the ulnar nerve as it passes through the cubital tunnel at the elbow. This is by far the most common site for entrapment. The cubital tunnel is a narrow passageway formed by bone, muscle, and ligaments. Because there isn’t much soft tissue protecting the nerve here, it’s vulnerable to pressure. Leaning on your elbows for long periods-like resting them on a hard desk while working or holding a phone to your ear for too long-can stretch and compress the nerve. About 90% of ulnar neuropathy cases occur at the elbow.
The second location is Guyon's Canal Syndrome, which refers to ulnar nerve compression at the wrist within a small space known as Guyon's canal. This is less common but often linked to repetitive trauma or pressure on the heel of the hand. Cyclists who rest their hands heavily on handlebars, golfers, and people who use vibrating tools are at higher risk. In some cases, a ganglion cyst or a fracture in the wrist bones can block the canal and squeeze the nerve.
| Feature | Cubital Tunnel (Elbow) | Guyon's Canal (Wrist) |
|---|---|---|
| Prevalence | Most common (~90%) | Less common |
| Common Triggers | Bent elbows, leaning on arms | Handlebar pressure, tool vibration |
| Nighttime Symptoms | Frequent (due to sleeping with bent elbows) | Less frequent |
| Structural Causes | Ligament thickening, arthritis | Ganglion cysts, hook of hamate fractures |
Recognizing the Signs: From Tingling to Claw Hand
Symptoms don’t appear all at once. They usually start mild and worsen over time if the underlying pressure isn’t relieved. Early on, you might notice intermittent numbness or tingling in your ring and little fingers. Many people describe it as a "pins and needles" feeling that comes and goes.
As the compression persists, the symptoms become constant. You may experience:
- Paresthesia: A burning or electric-shock-like sensation in the affected fingers.
- Weakness: Difficulty gripping objects, turning doorknobs, or using scissors. You might notice your hand feels clumsy.
- Froment Sign: When trying to pinch a piece of paper between your thumb and index finger, you unconsciously bend your thumb joint to compensate for weak muscles. This is a classic clinical sign of ulnar nerve damage.
- Muscle Atrophy: In advanced stages, the muscles between your knuckles shrink. Your hand may look thinner or develop a "clawed" appearance, especially in the fourth and fifth digits.
A key clue is timing. Symptoms often flare up at night. Why? Because most people sleep with their elbows bent. This position stretches the ulnar nerve across the elbow joint, increasing pressure inside the cubital tunnel. If you wake up shaking out your hand to restore feeling, ulnar neuropathy is a likely culprit.
Why Does This Happen? Risk Factors and Causes
Ulnar neuropathy isn’t random. Several factors increase your risk. Anatomical variations play a role-some people have tighter tunnels or extra bands of tissue that naturally compress the nerve. Repetitive motions are another major cause. Jobs requiring prolonged elbow flexion, such as plumbing, automotive repair, or even long hours on the phone, put continuous stress on the nerve.
Medical conditions also contribute. Diabetes can make nerves more susceptible to injury. Arthritis in the elbow or wrist can create bone spurs that press against the nerve. Previous injuries, like a broken elbow or wrist, can leave scar tissue that narrows the pathway. Interestingly, men are slightly more likely to develop this condition than women, with peak incidence occurring between ages 35 and 64.

Non-Surgical Therapies: First-Line Defense
For most patients, especially those with mild to moderate symptoms, conservative treatment works wonders. According to NIH research, nonsurgical management succeeds in relieving symptoms for about 50% of all patients, and up to 90% of those with mild cases. Here’s how doctors typically approach initial therapy.
1. Activity Modification
The simplest change can make the biggest difference. Avoid leaning on your elbows. Keep your arms straighter when possible. If you work at a desk, consider using an ergonomic mouse or keyboard that allows your forearm to rest flat rather than hanging off the edge. Take frequent breaks from activities that require repetitive gripping or bending.
2. Nighttime Bracing
This is often the game-changer. Wearing an elbow splint at night keeps your elbow straight or slightly bent (around 45 degrees), preventing the nerve from stretching during sleep. Studies show that consistent use for 4-6 weeks significantly reduces nighttime pain and morning numbness. Some patients need full-time bracing during acute phases, but night-only is usually sufficient for maintenance.
3. Medications
Over-the-counter nonsteroidal anti-inflammatory drugs (NSAIDs) like ibuprofen or naproxen can help reduce swelling around the nerve, particularly if symptoms started recently. For persistent nerve pain, doctors may prescribe medications like gabapentin or pregabalin, which target nerve signaling specifically. Corticosteroid injections around the nerve can also provide temporary relief by reducing local inflammation.
4. Physical Therapy and Nerve Gliding
A certified physical therapist can teach you nerve gliding exercises. These gentle movements help the ulnar nerve slide smoothly through its surrounding tissues, preventing adhesions. Patients typically perform these exercises 3-4 times daily. Therapy also includes strengthening exercises for the shoulder and forearm to improve overall biomechanics and reduce strain on the nerve.
When Surgery Becomes Necessary
If conservative treatments fail after several months, or if you already have significant muscle wasting or severe weakness, surgery might be the next step. Surgery aims to relieve pressure on the nerve. There are three main approaches:
- Simple Decompression: The surgeon cuts the tight ligament forming the roof of the cubital tunnel, giving the nerve more room. This is minimally invasive and has a faster recovery.
- Anterior Transposition: The nerve is moved from behind the elbow to the front, where it’s protected by muscle and fat. This is useful if the nerve subluxates (snaps out of place) when you bend your elbow.
- Medial Epicondylectomy: Part of the bony bump on the inner elbow is removed to create more space. This is less common today due to potential instability risks.
Recovery varies. Simple decompression may take 6-12 weeks, while transposition can require 3-6 months for full healing. Hand therapy usually begins 2-3 weeks post-op. While surgery is effective, about 12.5% of patients experience symptom recurrence if the underlying mechanical cause isn’t fully addressed. Therefore, choosing the right procedure based on your specific anatomy is crucial.

New Developments in Treatment
Medical science doesn’t stand still. Recent advancements offer new hope for patients. Ultrasound-guided nerve hydrodissection is emerging as a promising nonsurgical option. This technique involves injecting fluid under ultrasound guidance to separate the nerve from surrounding scar tissue, effectively creating more space without cutting. Early studies show positive results for select patients.
Researchers are also exploring biologic therapies like platelet-rich plasma (PRP) injections. PRP uses your own blood components to promote healing and reduce inflammation. However, evidence is still limited to small case series, so it’s not yet a standard recommendation. Minimally invasive endoscopic techniques are being developed to reduce postoperative pain and speed up recovery compared to traditional open surgeries.
Prognosis: What Can You Expect?
The outlook for ulnar neuropathy is generally positive if caught early. With appropriate treatment, approximately 85-90% of patients achieve satisfactory functional outcomes without permanent disability. The key is timing. Once muscle atrophy sets in, recovery is slower and sometimes incomplete. That’s why early diagnosis matters so much.
If you suspect you have ulnar neuropathy, don’t wait for it to "go away." Start with simple changes: stop leaning on your elbows, try a night splint, and consult a healthcare provider. They can perform tests like nerve conduction studies to confirm the diagnosis and rule out other issues, such as cervical radiculopathy (pinched nerve in the neck). Taking action now protects your hand function for the future.
How long does it take for ulnar neuropathy to heal with conservative treatment?
Most patients see improvement within 4 to 6 weeks of starting conservative therapy, including bracing and activity modification. However, complete resolution can take several months depending on severity. If symptoms persist beyond 3 months despite consistent treatment, surgical evaluation is recommended.
Can ulnar neuropathy cause permanent damage?
Yes, if left untreated for a long time. Chronic compression can lead to irreversible muscle atrophy and permanent sensory loss. Early intervention is critical to prevent long-term disability. Once muscle wasting occurs, recovery is difficult even after successful surgery.
Is cubital tunnel syndrome the same as carpal tunnel syndrome?
No. Carpal tunnel syndrome affects the median nerve at the wrist, causing numbness in the thumb, index, and middle fingers. Cubital tunnel syndrome affects the ulnar nerve at the elbow, impacting the ring and little fingers. They require different treatments and affect different parts of the hand.
What exercises help with ulnar nerve entrapment?
Nerve gliding exercises are most beneficial. These involve gently moving your arm, elbow, and wrist through specific positions to encourage the nerve to slide freely. Stretching the triceps and forearm muscles also helps. Always learn these from a physical therapist to avoid aggravating the nerve.
Should I wear an elbow brace during the day or only at night?
Nighttime bracing is the standard first-line treatment because symptoms often worsen during sleep due to elbow flexion. Daytime bracing is usually reserved for severe cases or jobs requiring repetitive elbow bending. Prolonged daytime use can weaken arm muscles, so follow your doctor’s advice.