
Imagine waking up, rolling over to hit the snooze button, and suddenly feeling like the entire room is spinning in a violent whirlwind. For a few seconds, you can't tell which way is up, and you feel a wave of nausea hit you. Then, just as quickly as it started, the world stops spinning, and you're left feeling shaky and confused. This isn't a stroke or a brain tumor-it's likely BPPV is a common inner ear disorder characterized by brief episodes of vertigo triggered by specific head movements. Also known as Benign Paroxysmal Positional Vertigo, it's the most frequent cause of peripheral vertigo worldwide.
While the word "benign" means it isn't life-threatening, that doesn't make the experience any less terrifying. When you're clutching the edge of the bed to keep from falling, it doesn't feel benign. The good news is that BPPV is a mechanical problem with a mechanical solution. You don't usually need heavy medication or surgery; you just need to get a few tiny "crystals" back where they belong.
What's Actually Happening in Your Ear?
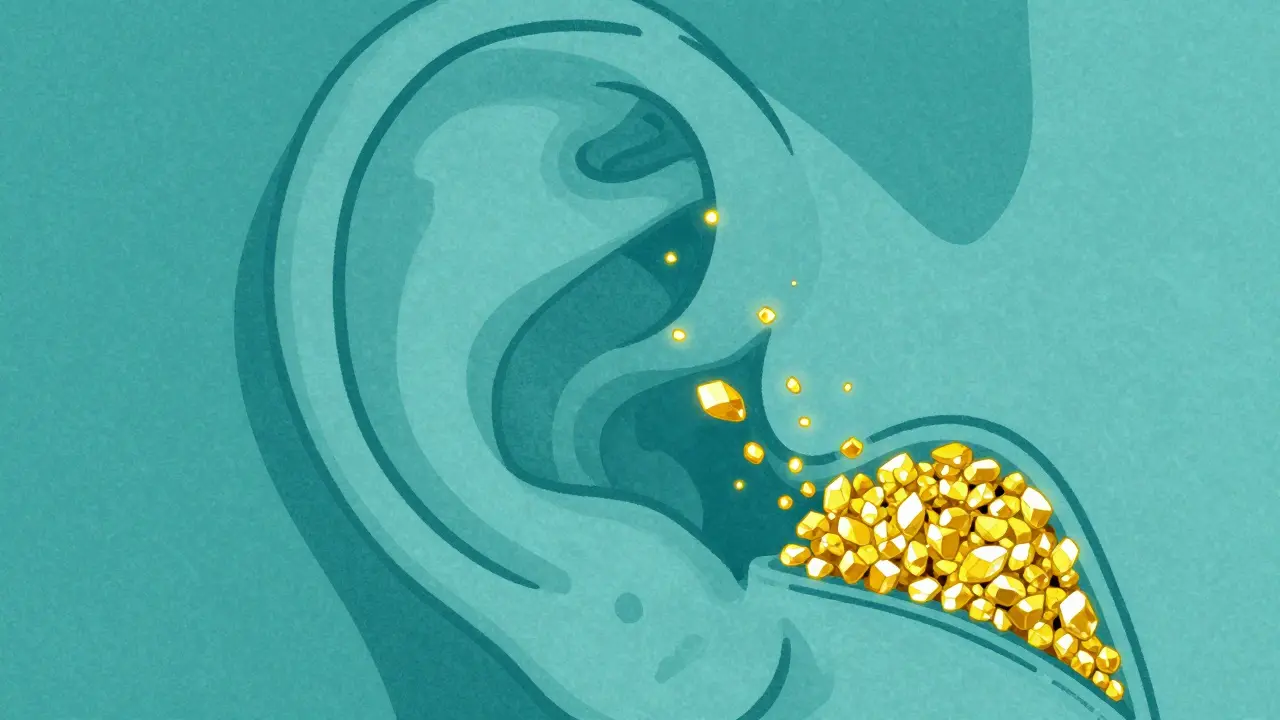
To understand why the room spins, we have to look at the Vestibular System, which is your body's internal gyroscope. Inside your inner ear, you have three semicircular canals filled with fluid. These canals help you keep your balance by sensing rotation. To help these canals work, your ear uses tiny calcium carbonate crystals called Otoconia. Normally, these crystals stay put in a specialized area called the utricle.
BPPV happens when these crystals break loose and drift into one of the semicircular canals. Think of it like a grain of sand getting into a delicate watch mechanism. When you move your head, these loose crystals shift and push the fluid in the canal. This sends a false signal to your brain that you're spinning, even though your eyes see that you're standing still. This conflict between your eyes and your inner ear is what creates that dizzying sensation.
In about 80-90% of cases, the crystals end up in the posterior semicircular canal. However, some people experience a different version where crystals enter the horizontal canal, which often feels more like a side-to-side shift rather than a vertical spin.
Spotting the Signs: Is It BPPV or Something Else?
Not all dizziness is created equal. If you're trying to figure out if your vertigo is BPPV, look for these specific patterns. BPPV episodes are usually very short-typically lasting between 5 and 30 seconds, and almost always under one minute. They are also "positional," meaning they only happen when you move your head in a certain way. Common triggers include:
- Rolling over in bed (the most common trigger for 85% of patients)
- Looking up at a high shelf
- Bending over to tie your shoes
- Tipping your head back at the dentist
You might also notice Nystagmus, which is a fancy term for involuntary, rhythmic eye movements. While you might not see this yourself, a doctor will look for it during a diagnosis because the way your eyes jump tells them exactly which canal the crystals are stuck in.
It's important to distinguish BPPV from other issues. For instance, Meniere's disease usually involves hearing loss and ringing in the ears (tinnitus), and vestibular neuritis causes a constant spin that lasts for days. If you have a sudden onset of vertigo accompanied by a severe headache, slurred speech, or numbness, that's a medical emergency and could be a stroke-not BPPV.
The Gold Standard: The Dix-Hallpike Test
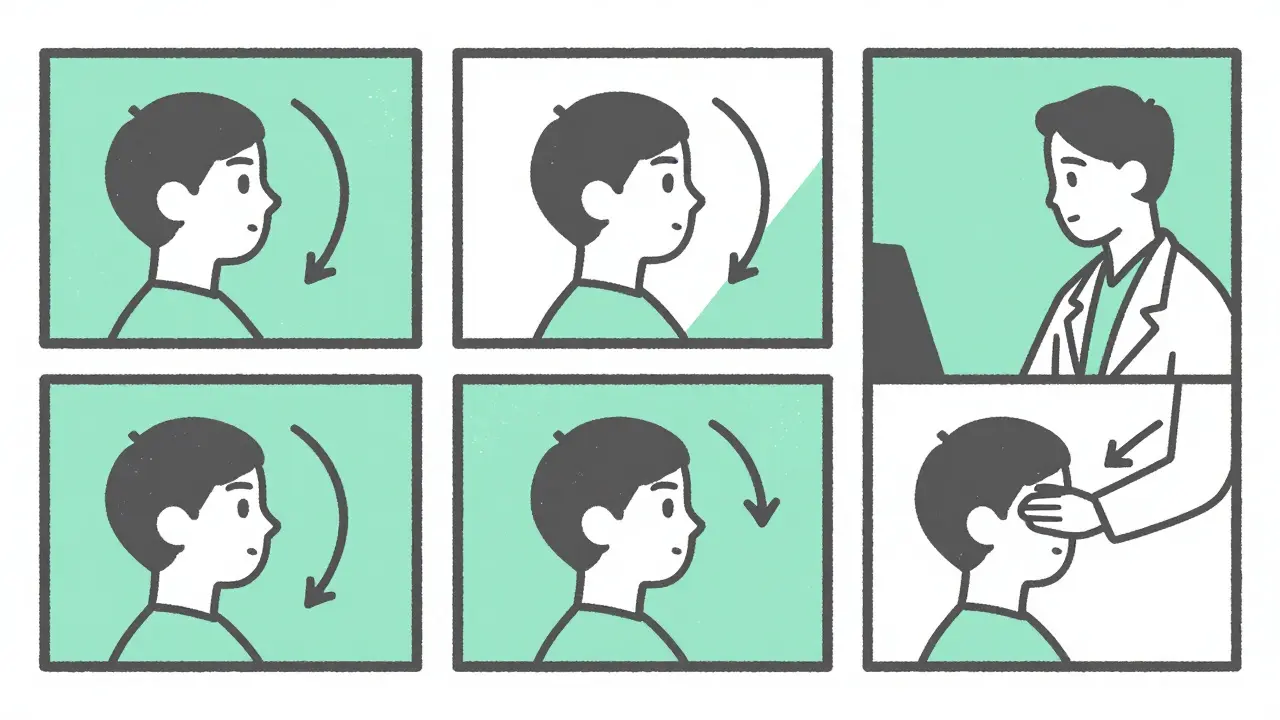
How does a doctor prove you have BPPV without using an MRI? They use a physical test called the Dix-Hallpike maneuver. During this test, the provider will have you sit up, turn your head 45 degrees, and then quickly lay you back with your head hanging slightly off the edge of the table.
If you have BPPV, this movement shifts the loose crystals, triggering a brief episode of vertigo and a specific eye-fluttering pattern. It's a bit disconcerting to experience the spin again, but it's the only way to confirm which ear and which canal are affected. Research shows that this physical exam is far more accurate for diagnosing BPPV than an MRI, which often comes back normal even when the patient is suffering.
Fixing the Spin: Canalith Repositioning
Since the problem is a physical blockage of crystals, the cure is to physically move them out. This is called canalith repositioning. The goal is to use gravity to guide the crystals out of the semicircular canal and back into the utricle where they belong.
| Maneuver | Target Area | Typical Success Rate | Best For |
|---|---|---|---|
| Epley Maneuver | Posterior Canal | 80-90% | Standard vertical vertigo |
| Semont Maneuver | Posterior Canal | 85% | Patients who can't tolerate Epley |
| Lempert Roll | Horizontal Canal | 75% | Side-to-side spinning |
| Brandt-Daroff | General Vestibular | 50% | Home habituation exercise |
The Epley maneuver is the most famous of these. It involves a series of three or four head positions, each held for about 30 to 60 seconds. By rotating the head in a specific sequence, the doctor "rolls" the crystal through the canal and back into the center of the ear. Many people find that their vertigo vanishes almost instantly after a single session.
If you're attempting this at home via a video tutorial, be careful. If you move your head into the wrong position, you can actually push the crystals deeper into the canal or move them into a different one, making the vertigo worse or harder to treat. Professional guidance is always safer.
Life After BPPV: Recurrence and Prevention
One of the most frustrating things about BPPV is that it can come back. About 15% of people see it return within a year, and up to 50% may experience it again within a decade. Why? Sometimes the crystals just aren't "sticky" enough to stay in place, or the inner ear structure is slightly more prone to leakage.
Interestingly, some recent data suggests a link between BPPV and Vitamin D deficiency. Because otoconia are made of calcium, a lack of Vitamin D might make them more likely to break off. Some patients have found that a daily supplement of 1,000 IU of Vitamin D helps reduce how often the vertigo returns.
For those who suffer from chronic recurrence, vestibular rehabilitation therapy (VRT) can be a lifesaver. This isn't about moving the crystals, but rather training your brain to ignore the false signals. By performing specific exercises, your brain learns to rely more on your vision and touch and less on the glitchy signals coming from your inner ear.
Common Mistakes in BPPV Management
Many people make the mistake of treating BPPV with medication. You'll often see prescriptions for vestibular suppressants like meclizine. While these can stop the feeling of nausea, they don't actually fix the problem. In fact, using these drugs for too long can actually slow down your recovery because they prevent your brain from adapting to the imbalance.
Another common pitfall is the "wait and see" approach. Some people hope the crystals will just dissolve on their own. While spontaneous resolution happens in about 40-50% of cases within a month, the repositioning maneuvers offer a much faster and more reliable fix. Waiting months for a diagnosis often leads to unnecessary anxiety and a fear of falling, which can actually limit your mobility and overall health.
Can I treat BPPV at home?
Yes, many people use the modified Epley maneuver at home. However, the success rate is lower (around 72%) compared to professional treatment. The risk is that if you perform the movement incorrectly, you may push the crystals into a different canal, making the vertigo more complex to treat. It is highly recommended to get a professional diagnosis first to ensure you're treating the correct canal.
How long does it take for BPPV to go away?
If left alone, BPPV can last for weeks or months. However, with a successful canalith repositioning procedure like the Epley maneuver, 95% of cases resolve within two weeks. In many instances, the spinning stops immediately after the first session, though you may feel some lingering imbalance for a few days.
Does BPPV cause permanent hearing loss?
No. BPPV only affects the balance portion of the inner ear. It does not involve the cochlea (the hearing organ), so it does not cause hearing loss or tinnitus. If you are experiencing vertigo along with hearing loss, you should be screened for Meniere's disease or other vestibular disorders.
Why does the room spin only when I turn my head?
This is because the loose otoconia (crystals) only move when gravity pulls them. When your head is still, the crystals are stationary. When you tilt or turn your head, the crystals slide through the fluid in the semicircular canal, which triggers the false sensation of movement in your brain.
Is there a way to prevent BPPV from coming back?
While there is no guaranteed way to prevent it, some evidence suggests that maintaining healthy Vitamin D levels can reduce the fragility of the crystals. Additionally, practicing balance exercises and maintaining general inner ear health through regular check-ups can help you manage the condition if it does recur.
